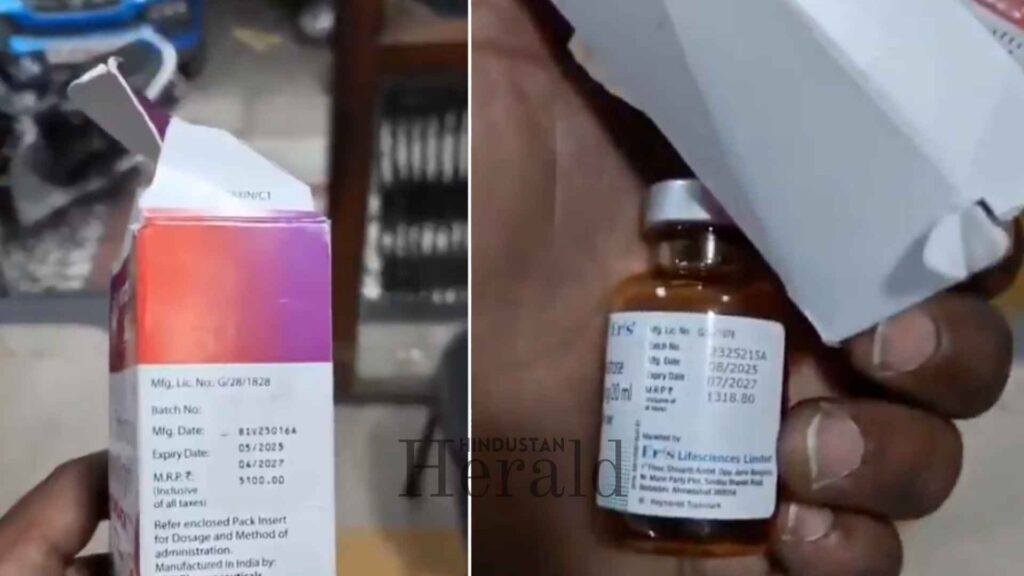
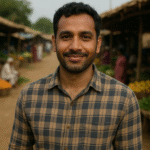
New Delhi, May 8: The box placed over the box tells the whole story. An injection with a Maximum Retail Price (MRP) of roughly Rs 1,300 printed on its original packaging. A second box slipped over the first, bearing a fresh price of Rs 5,100. The patient’s family, already running between wards and billing counters, has no idea. The medicine goes in. The inflated amount goes into the hospital’s ledger. And by the time anyone realises what has happened, the treatment is over, the discharge papers are signed, and the bill has been paid.
This is not a stray incident reported from some obscure corner of the country. It is a pattern, deliberate and systemic, that plays out daily across the private healthcare sector in India. The method changes; the result does not. Families already battered by fear and uncertainty walk into hospitals seeking care and walk out carrying debt.
When the Packaging Becomes the Weapon
There is something uniquely calculated about using a second box to hide the original MRP. It is not sloppy billing. It is not a clerical error. It requires someone to physically obtain outer packaging, place it over the original, and then present that figure to a patient who has no bandwidth to verify anything at a moment of medical crisis.
Private hospitals have been documented charging five times the MRP on disposable items, with cases of gloves billed at Rs 2,500 and IV cannulas billed at several multiples of their actual cost. The injection overcharging tactic described above fits neatly into this category. The patient’s vulnerability is not incidental to the scheme. It is load-bearing.
In Ludhiana earlier this year, relatives of a patient accused a private hospital’s in-house pharmacy of selling an injection that cost Rs 500 at Rs 7,500. When the family objected, staff agreed to bring it down to Rs 5,000 through what amounted to bargaining at a hospital counter. The incident escalated into a public protest. That same injection was available at local pharmacies for its actual price. The hospital had simply decided that distress was a pricing opportunity.
The Anatomy of a Rigged Bill
Understanding how this happens requires looking at how private hospital billing actually works in India. Most families, when they arrive at a hospital in a crisis, sign consent forms they cannot read carefully, agree to package deals they do not fully understand, and pay for items they are never shown. The bill arrives at the end, itemised in ways designed to be opaque rather than transparent.

Investigations have found that hospitals in some cases charge between 10 and 30 times the actual cost of certain medical consumables. A syringe costing roughly Rs 3 may be billed at Rs 30. An IV cannula with a base cost of around Rs 6 has been billed at up to Rs 120. For high-value devices, the gap widens further, with pacemakers costing around Rs 25,000 reportedly billed close to Rs 2 lakh, and imported heart valves costing about Rs 4 lakh billed as high as Rs 26 to 30 lakh.
The injection case that sparked this story sits at the more modest end of that spectrum, and that is precisely what makes it so telling. This is not a Rs 30 lakh heart valve. This is a routine injection. If the markup on something this ordinary can reach nearly four times its MRP, what is happening to the items patients cannot easily track, compare, or question?

The issue of pricing becomes especially acute in a healthcare market that operates under highly competitive to oligopolistic conditions, where the patient has no practical power to negotiate or walk away. You do not shop around for hospitals when your family member’s oxygen saturation is falling.
A Regulatory Vacuum That Was Never Accidental
India has known about this problem for a long time. The Clinical Establishments Act was passed in 2010, designed to regulate hospitals, clinics, and diagnostic centres and bring some accountability to private healthcare. More than fifteen years later, its implementation remains patchy at best.
United Andhra Pradesh was among the first states in India to enact a Clinical Establishments Act as far back as 2000. Rules were framed in 2005. The Act was never enforced, with politicians citing fears of promoting “inspector raj” as justification. That same political reluctance has echoed across states ever since.

Rajya Sabha MP Swati Maliwal raised this issue pointedly during Zero Hour in Parliament earlier this year, drawing attention to how many private hospitals have gradually shifted away from their original role as healthcare providers. She warned that unchecked overcharging is transforming healthcare into a source of long-term economic instability for families, particularly the middle class.
Maliwal’s concerns were not framed as isolated complaints. They were framed as a systemic failure, one in which billing opacity, weak insurance protections, and the absence of meaningful oversight have created a private healthcare environment where the sickest and most desperate pay the most.
The Insurance Trap
One dimension of this crisis that rarely gets enough attention is how health insurance has, paradoxically, made overcharging easier. When a patient is insured, the psychological barrier to questioning a bill weakens. The family assumes the insurer will handle it. The hospital, knowing a third party is paying, has even less incentive to keep costs down.
Health insurance claims in India have seen a notable uptick in recent years, which has intensified the need for more structured billing practices. Rising hospital costs are now directly straining the insurance ecosystem, pushing premiums upward and reducing the reliability of coverage for ordinary policyholders.
Medical inflation in India is currently running between 11 and 15 percent annually, far outpacing general inflation. This rise in healthcare costs is directly driving up health insurance premiums by 10 to 15 percent per year. The family that bought insurance to protect itself from financial ruin from a medical emergency is now watching that protection erode, quietly, every renewal cycle.
What the Government Is Now Considering
The scale of the problem has finally pushed the conversation toward regulatory action. As per sources cited by multiple outlets, the Union Health Ministry is currently examining a proposal to cap the trade margins that hospitals can charge on medical devices and consumables.
The government is evaluating a framework under which hospitals would not be allowed to bill beyond a fixed percentage over the cost or landing price of medical products. The proposed cap may cover everyday consumables such as syringes, cannulas, and gloves, as well as high-value devices including pacemakers and heart valves.
Discussions within policy circles suggest a cap of somewhere between 30 and 50 percent for specific devices, with a 2018 NITI Aayog proposal having previously recommended a ceiling of around 65 percent.
Officials are reportedly consulting stakeholders from the medical device industry and the insurance sector to assess how such a cap could be structured without creating perverse incentives or pushing costs into other billing categories. That last concern is not paranoia. It is based on precedent. When the government capped prices on cardiac stents a few years ago, some hospitals responded by inflating charges under other heads. The system has a long memory for workarounds.
Still, the direction is significant. That the government is even formally examining margin caps on consumables marks a shift from a posture of non-interference that has defined healthcare regulation for decades.
The Hidden Cost of Helplessness
What makes this crisis morally distinct from ordinary price gouging is the condition under which it occurs. The patient lying on the hospital bed is not choosing between competing products. They are not in a position to negotiate. They cannot walk out. Their family is managing fear, logistics, and paperwork simultaneously.
A single medical emergency can erase years of savings, force families into debt, or require the sale of assets. This pattern functions as a systemic distortion where profit motives overshadow patient-centric care.
Under the Consumer Protection Act of 2019, hospitals are classified as service providers, which means patients can legally pursue action for overcharging and mental harassment. Consumer district commissions handle claims under Rs 50 lakh, state commissions handle claims up to Rs 2 crore, and the national commission handles cases above that threshold. In practice, most families do not pursue these channels. The process takes anywhere from six to eighteen months, requires documentation that was never collected in the chaos of hospitalisation, and demands emotional energy from people who are still recovering from the crisis itself.
In the current legal environment, apart from filing a case in consumer court or approaching a civil court, there is no immediate relief available for overcharging. That is the core of the problem. The deterrent does not operate in real time. By the time any accountability arrives, the hospital has long moved on.
What Accountability Would Actually Look Like
Genuine reform in this space would require several things working together. Price caps on consumables and devices are necessary but not sufficient. Hospitals need to be required to display itemised pricing before treatment begins, not after. The MRP on every product administered to a patient should be recorded in the bill, with any markup explicitly justified. Third-party billing auditors, funded by regulators rather than hospitals, would be one model worth examining.
Private healthcare providers in India are unusual among commercial service sectors in that rates are generally not available in the public domain, and wide variations exist not just between hospitals but between different patients within the same hospital for the same procedure. This opacity is not a market characteristic. It is a policy failure dressed up as complexity.
Some states have taken steps in isolation. Tamil Nadu and Rajasthan have experimented with centralised procurement of generic medicines to cut out inflated supply chain margins. But these remain exceptions rather than the norm, and they do not address the full range of consumables and devices that form the bulk of inflated hospital bills.
For Now
The injection in the second box represents something simple to understand and deeply difficult to fix. It is a symptom of a system in which the patient has no leverage, the regulator has no presence, and the family at the bedside is too consumed by grief and fear to read fine print.
As it turns out, change requires more than scandal. Every few months, a story like this surfaces, provokes outrage, draws statements from officials, and then fades. The families who were overcharged move on, poorer and quieter. The hospitals continue functioning.
The proposed margin caps, if they materialise into enforceable rules rather than another consultation paper, would represent the first meaningful structural intervention in years. But until the second box placed over the first MRP becomes legally impossible to present to a patient, the problem will persist. Quiet, routine, and very profitable.
Stay ahead with Hindustan Herald — bringing you trusted news, sharp analysis, and stories that matter across Politics, Business, Technology, Sports, Entertainment, Lifestyle, and more.
Connect with us on Facebook, Instagram, X (Twitter), LinkedIn, YouTube, and join our Telegram community @hindustanherald for real-time updates.
Regional journalist bringing grassroots perspectives and stories from towns and cities across India.
- Sandeep Verma

- Sandeep Verma
- Sandeep Verma
- Sandeep Verma



